Editor’s intro: Drs. James E. Eckhart and Thikriat Al-Jewair delve into mandibular growth in boys and girls and how it relates to tooth movement and chin growth.
Drs. James E. Eckhart and Thikriat Al-Jewair quantify how much the mandibles of untreated pubertal boys and girls grow per month and show how certain growth of the chin is related to how the incisors change positions during that growth
Abstract
Objective

To quantify how much the mandibles of untreated pubertal boys and girls grow per month and to show that the horizontal and vertical expression of that growth of the chin is related to how the incisors change positions during that growth.
Materials and methods
Lateral cephalograms from untreated deep-bite Class II boys and girls chosen to be of pubertal age were selected. Films were approximately 2 years apart. The films were fiducialized, and landmarks were drawn on the T1 film and transferred to the T2 film by one experienced investigator. Changes in upper and lower incisor positions and gnathion were measured for both vertical and horizontal components. The average monthly radial movement of gnathion was calculated, and the relation between incisor movements and gnathion horizontal and vertical movement was graphed.
Results
For boys, the average radial monthly movement of gnathion was 0.27 mm/mo. For girls, it was 0.18 mm/mo. The horizontal and vertical movements of the lower incisor were then subtracted from the horizontal and vertical movements of the upper incisor, and that sum was graphed against the ratio of the gnathion horizontal movement vector (or the gnathion vertical movement vector) to the gnathion radial movement vector, and a near-linear relationship was found for both boys and girls.
Conclusions
The percentage horizontal growth (and vertical growth) changes in gnathion is related approximately linearly to the sum of horizontal and vertical growth movements of the upper and lower incisors. Pubertal untreated boys grow the chin 50% more than pubertal girls.
Introduction

It is common to see articles showing chosen cases of Class II correction in as few as 6 months, documented by photos showing before-and-after buccal occlusion. Occasionally, an article also shows single-case superimposed head film tracings demonstrating the profile change resulting from the Class II correction. It is much less common to consider the question of how the chin profile of a group of treated persons compared to that of a similar untreated group of persons. We are presenting here information about the normal pubertal chin growth of untreated Class II boys and girls, so that other papers can compare the pubertal chin growth of a group of treated Class II boys and girls to these control groups. Therefore, the teen subjects in this paper are referred to as “controls,” even though they are not compared to a treated group in this paper.
It is reported to be possible to increase mandibular growth compared to what would have occurred in untreated controls, using mandibular advancers, provided that the treatment occurs during puberty, and provided that the treatment period be long enough duration,1,2,3,4 but it has not been specifically reported how much the mandible grows per month during puberty in control boys and control girls. We have studied herein one group each of untreated boys and girls to establish gnathion growth information for untreated “controls.” It has been reported that the horizontal/vertical growth repositioning of the chin depends on the amount and direction of condylar growth, the amount and direction of glenoid fossa growth, and other factors that control the rotation of the mandible.5 Few if any papers have discussed the relationship between incisor position changes and horizontal/vertical chin profile changes, in controls or in treated groups. It has been published that the pubertal period averages 30 months, during which the unassisted mandibular growth rate averages 59% higher for boys and 34% higher for girls than the pre-puberty average of 2.4-2.1 mm per year.6
If the optimum time to try to improve horizontal chin projection is during pubertal growth, correctly estimating the timing of the pubertal growth is important. Mellion, et al.’s6 study of untreated pubertal teens (most of whom were not Class II’s), showed that peak mandibular growth in boys averages 4 months later than their peak statural growth, and for girls the peak mandibular growth rate averages 7 months later than their peak statural growth.6 The study showed that boys begin the mandibular growth spurt at an average age 11.9, and girls begin it at an average age 9.5, leading us to conclude that because of the pubertal age differences and the mandibular growth magnitude differences, mixing sexes in selection of control groups and clinical trials should be avoided. Historically, the reason studies have mixed girls with boys may have been the difficulty in finding large enough samples of untreated Class II control girls in the proper age range.
This retrospective study aims to quantify how much the mandibles of untreated pubertal boys and girls grow per month, and to show that the horizontal/vertical expression of that growth is related to how the incisors change positions during that growth.
As shown in Figures 1 and 2, drawings of the mechanics of mandibular growth7 suggest that the horizontal/vertical components of gnathion growth depend on how the upper and lower incisors move (in deep bites), because the drawings show that extrusion and retraction of the upper incisor, whether by orthodontic movement within the maxilla or by orthopedic movement of the maxilla, or both, is accompanied by downward vertical rotation and some backward rotation of the chin, and extrusion and protraction orthodontic movement of the lower incisor increases vertical rotation of the growing chin.
Materials and methods
This is a retrospective study of a sample of untreated boys and girls obtained from the Michigan and Bolton-Brush growth studies.8 We selected Class II boys and girls but excluded open bites because of our intention to test the relationship of incisor change to horizontal chin change. As shown in Table 1, for 24 boys, the average T1 age was 13.2 years, and the average T2 age was 15.2 years. The average film interval was 24.6 ± 3.6 months, range 21-39 months. For 15 girls, the average T1 age was 10.6 years, and the average T2 age was 12.9 years. The average film interval was 28.4 ± 8.8 months, range 12-38 months.
Table 1: There were 24 boys aged 13.2 ± (-.0.3, +1.0) years, measured over 24.6 ± (-3, +15) months. There were 15 girls aged 10.6 ± (-0.7, +1.2) years, measured over 28.4 ± (-16, +8) months.
In selecting a method to assess pubertal status, we chose Mellion’s chronological age method. Gabriel, et al.,9 reported poor reliability between observers using the CVM10 method, and Mellion6 reported that the CVM method was the least reliable at predicting pubertal growth spurts. This paper shows distinct results of boys and girls control selections.
In both (boys and girls) control groups, the T1 and T2 digital films were fiducialized and corrected for known magnification, per published reports.11 Lines were drawn on the T1 film for SN, S-A, S-U1, S-Gn, palatal plane, and functional occlusal plane (Figure 3A). Also, the incisal tip of L1 was marked, and three dots circumscribed sella. These points were chosen because they are easy midline structures to identify accurately. Although many published studies measured Co-Gn or Ar-Gn to assess mandibular length, we found to be easier to see S-Gn when comparing two films. This method had a small error of overlooking glenoid fossa growth, which we chose to ignore due to its small magnitude and due to the short T1-T2 intervals. Mandibular radius was approximated to be from sella to gnathion for both T1 and T2, wherein only the change in gnathion was examined.

Then the T1 lines and dots were grouped, copied and pasted (Figure 3B), and transferred to the T2 film and superimposed on SN at S (Figure 3C). Sometimes the T2 film had to be rotated in PowerPoint so the grouped lines would superimpose correctly on SN, depending on the variation in tip angle of the head between T1 and T2. The T2 A pt, U1, L1, and Gn were then marked and grouped onto the T2 film (Figure 3C).
Next, the incisor changes and gnathion change (ΔU1, ΔL1, and ΔGn) were measured in their X and Y distances from the T1 U1, L1, and Gn, using the T1 occlusal plane as the reference X axis (Figures 4A-4C) . The Δ measurements were made by viewing the films at 200% to increase accuracy, and then correcting the tables to 100% in Excel.
As shown on the legend for Table 2, we measured the X and Y changes of the upper incisor, the lower incisor, and gnathion, for 24 boys and 15 girls, over a period of a little more than two years.
Results
- Note that as shown in Table 3, the lower dentition of the control boys moved backward 0.4 mm in 24.5 months, or -0.02 mm/month.
- Average ∆Gn of all control boys = 0.27 mm/month during peak mandibular growth.
- Average ∆GnX of all control boys = 0.17 mm/month.
- Average ∆GnY of all control boys = 0.22 mm/month.
- The lower dentition of the control girls moved backward 0.8 mm in 28.4 months, or -0.03 mm/month
- Average ∆Gn of all control girls = 0.18 mm/month during peak mandibular growth.
- Average of all control girls GnX = 0.12 mm/month.
- Average of all control girls GnY = 0.14 mm/month.
Note that in controls, the pubertal chin growth has a higher vertical component than horizontal component. For clarity, the Table 3 entries called “AVG ∆U1-∆L1” should more accurately be called “AVG (∆U1X + ∆U1Y – ∆L1X – ∆L1Y).
For control boys and girls, the sum of the upper incisor X and Y movements, minus the sum of the lower incisor X and Y movements was related linearly to the proportion of chin growth that was horizontal and to the proportion of chin growth that was vertical. For control boys, the Pearson correlation coefficient was r = 0.8262, and the probability factor was p = < 0.00001. The result is significant at p < 0.05. For control girls, the Pearson correlation coefficient was r = 0.8081, and the probability factor was p = 0.000267. The result is significant at p < 0.05.
Movements of the upper incisor forward and upward tend to accompany the horizontal expression of growth at gnathion, and movements of the lower incisor downward and backward also appear to accompany the horizontal expression of growth at gnathion. As shown in the Figure 5 graphs, the sum of the upper incisor movements in x and y direction, minus the sum of the lower incisor movements in x and y direction, is approximately related linearly to the percent of mandibular radial growth which is expressed in the horizontal (x) direction (x being the T1 occlusal plane). Conversely, the same sum of incisor movements is also related linearly to the percent of mandibular radial growth which is expressed in the vertical (y) direction.
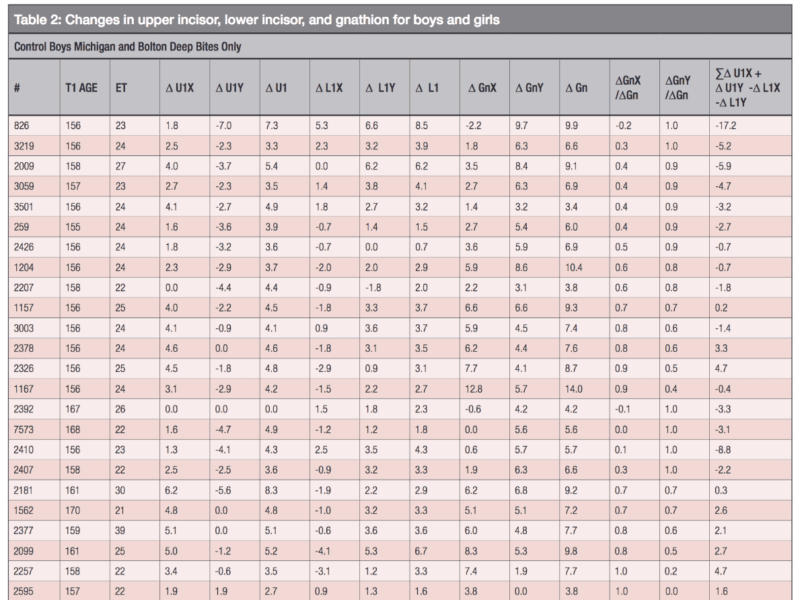
# = control patient ID number from Bolton or Michigan
T1 AGE = age of patient in months at time point 1
ET = number of months between film 1 and film 2
∆U1X = change of upper incisor position between films, parallel to T1 occlusal plane, films superimposed on Sella-
Nasion at Sella (SN at S)
∆U1Y = change of upper incisor position between films, perpendicular toT1 occlusal plane, films superimposed on SN at S
∆U1 = vector distance of change of upper incisor tip position between films, films superimposed on SN at S
∆L1X = change of lower incisor distance from its own Gnathion between films, parallel to T1 occlusal plane, super-imposed on SN at S
∆L1Y = change of lower incisor distance from its own Gnathion between films, perpendicular to T1 occlusal plane, superimposed on SN at S
∆L1 = vector distance of change of lower incisor tip position from its own Gnathion between films, films superimposed on SN at S
∆GnX = change of Gnathion position between films, parallel to T1 occlusal plane, films superimposed on Sella-Nasion
at Sella (SN at S)
∆GnY = change of gnathion position between films, perpendicular to T1 occlusal plane, films superimposed on sella-
nasion at sella (SN at S)
∆Gn = vector distance of change of Gnathion position between films, films superimposed on SN at S
∆GnX/∆Gn = percent of gnathion change between films which is parallel to T1 occlusal plane
∆GnY/∆Gn = percent of gnathion change between films which is perpendicular to T1 occlusal plane
∑= “the sum of
Discussion

Future authors in studying the effect of mandibular advancers on increasing mandibular radial growth in pubertal teens can assume that pubertal control boys would grow 0.27 mm/mo., and that pubertal control girls would grow 0.18 mm/mo., relative to superimposition on sella. Clinicians hoping to maximize horizontal chin profile expression may do well to avoid retracting or extruding upper incisors in deep bite cases. Clinicians hoping to maximize vertical chin profile expression may do well to retract and extrude upper incisors and avoid intruding or retracting lower incisors.
Conclusion
- For control boys, the mandibular growth was 0.27 mm/month, and it was 44% horizontal. (∆GnX/(∆GnX + ∆GnY))
- For control girls, the mandibular growth was 0.18 mm/month, and it was 46% horizontal. (∆GnY/(∆GnX + ∆GnY))
- Pubertal untreated boys grow the chin 50% more than pubertal girls.
- Because of the large mandibular growth rate difference between pubertal boys and girls, they should not be mixed in studies involving mandibular growth.
- The vertical component of untreated pubertal mandibular growth is larger than the horizontal component.
- For both boy and girl pubertal controls with deep-bite Class II’s, the upper incisor forward and upward movements, minus the lower incisor forward and upward movements (sum) was related linearly to the ratio between the horizontal vector of mandibular growth and the radial vector of mandibular growth, and also to the ratio between the vertical vector of mandibular growth and the radial vector.
- Incisal guidance seems at least to be related to direction of chin profile expression. The drawings of the mechanics involved suggest the relationship is causative.
For another article on mandibular growth — this time its relationship to nasal breathing, read Dr. Nelson Oppermann’s article, “The importance of nasal breathing and its effect on the direction of mandibular growth,” here.
- Freeman DC, McNamara JA Jr, Baccetti T, Franchi L, Fränkel C Long-term treatment effects of the FR-2 appliance of Fränkel. Am J Orthod Dentofacial Orthop. 2009;135(5):570.
- Rabie AR, She TT, Hägg U. Functional appliance therapy accelerates and enhances condylar growth. Am J Orthod Dentofacial Orthop. 2003;123(1):40-48.
- Malta LA, Baccetti T, Franchi L, Faltin K Jr, McNamara JA. Long-term dentoskeletal effects induced by bionator therapy. Angle Orthod. 2010;80(1):10-17.
- Franchi L, Pavoni C, Faltin K Jr, McNamara JA, Cozza P. Long-term skeletal and dental effects and treatment timing for functional appliances in class II malocclusion. Angle Orthod. 2013;83(2):334-340.
- Buschang PH, Jacob HB. Mandibular rotation revisited: What makes it so important? Semin Orthod. 2014;20(4):299-315.
- Mellion ZJ, Behrents RE, Johnston LE Jr. The pattern of facial skeletal growth and its relationship to various common indexes of maturation. Am J Orthod Dentofacial Orthop. 2013;143(6):845-854.
- Björk A. Prediction of mandibular growth rotation. Am J Orthod. 1969;55(6):585-599.
- AAOF Legacy Collection. https://www.aaoflegacycollection.org/aaof_home.html <incomplete citation>
- Gabriel DB, Southard KA, Qian F, et al. Cervical vertebrae maturation method: poor reproducibility. Am J Orthod Dentofacial Orthop. 2009;136(4):148.
- Baccetti T, Franchi L, McNamara JA Jr. The Cervical Vertebrae Maturation (CVM) Method for the Assessment of Optimal Treatment Timing in Dentofacial Orthopedics. Semin Orthod. 2005;11(3):119-129.
- Scaled Measurements from the AAOF Legacy Collection Images. https://www.google.com/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&cad=rja&uact=8&ved=0ahUKEwjTy6TSwJPWAhVp.mMKHdipB3kQFggmMAA&url=http%3A%2F%2Fwww.aaoflegacycollection.org%2FAAOF_Images%2FAAOFScaledMeasurement.pdf&usg=AFQjCNFtiRt9Miz_mtcWDhEJx5mX3DWXfA Accessed December 19, 2018.
Stay Relevant with Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
Read our following terms and conditions before subscribing.
