Dr. Mark McDonough discusses increasing efficiency through proper treatment decisions
Introduction
There has been a lot written in the orthodontic literature recently about efficiency related to types of braces, wires, clear aligners, vibrating devices, and micro-perforations all designed to increase the efficiency of tooth movement.
If you look at orthodontists’ websites, they will prominently display the names and logos of these braces and devices. My concern is that the focus on the type of appliance makes the orthodontist a marketing arm of the manufacturing companies. Once the orthodontist is considered simply to be an offshoot of these dental manufacturers, it is very easy for these same companies to market these appliances to general dentists. The public is easily confused about the difference between orthodontics and an orthodontist. The end result is that these companies are devaluing the specialized services of an orthodontist by changing the focus to the products or technology instead of the beneficial patient-focused profession that it is. This has already happened with Invisalign® (Align Technology) since general dentists currently provide more Invisalign treatment than orthodontists. The manufacturers’ marketing is designed to have the public look for a provider of their product instead of an orthodontist. As far as the public is concerned, they often want to be treated by an “insert the name of your favorite appliance” provider instead of a highly qualified dental specialist.
The message orthodontists should be marketing to the public is not that they are the providers of the latest technology but that they are the most qualified professionals to treat malocclusions and dental facial discrepancies. The greatest service we as orthodontists provide to our patients is our understanding of growth, development, force systems, timing, and a complete and an honest diagnosis and treatment plan. These skills are what make the orthodontist uniquely positioned to manage the often-complex needs of our patients. I am not trying to make a statement against the wonderful technological advances and the companies that promote them. I use many technological advances on a daily basis in my practice, and I am grateful to the companies that continue to push the envelope of efficient treatment. The take-home message for this article is that efficiency is primarily a product of proper treatment decisions, not necessarily technology decisions.
The following examples demonstrate how to efficiently manage moderate and severe crowding. You will see moderate crowding relieved prior to the placement of braces. You will see two 4-premolar extraction patients treated in 14 and 15 months, and an upper premolar extraction patient treated with Invisalign express in 5 months. You may expect to read about a breakthrough in a revolutionary new bracket or adjunctive therapy. The reality is our greatest efficiency is found through beginning treatment at the appropriate time while managing the growth and development of our patients and applying appropriate force systems. This is the message we need to promote to our dental colleagues and the public. This message will prevent orthodontists from becoming a commodity that is easily replaced. The greatest service to the future of our profession is to provide excellent results for our patients in the shortest treatment time at a reasonable cost. The following are a few examples to keep in mind when diagnosing and treatment planning. These concepts will improve your efficiency, create beautiful stable results, and save you money.
Leeway space and efficient treatment
Lower incisor crowding is one of the most prevalent chief complaints that present to the orthodontist. An efficient way to help relieve the mandibular crowding is by utilizing the leeway space. This concept was presented by Dr. Anthony Gianelly1, who showed that 4-5 mm of mandibular incisal crowding could routinely be relieved by utilizing a passive lingual holding arch. He demonstrated that the increase in arch length was due to a combination of the leeway space, growth, and development. The following patient is a typical late-mixed dentition adolescent who was referred to our office for evaluation of the lower incisor crowding (Figures 1 and 2). A mandibular lingual holding arch was fabricated, and 11 months later she was ready for fixed appliances. The ideal time to place the lower lingual holding arch is approximately 4 to 12 months prior to loss of the first mandibular primary molar. Once the patient enters the adult dentition, the crowding has resolved (Figure 3).

Due to our focus on efficiency, we have developed a simple method to fabricate soldered appliances. We are able to complete records, separators, case presentation, fabrication of the soldered appliance, and insertion in two visits. On the first visit, full orthodontic records, including study models, are taken, and the appropriate separators are placed. When they returned 1 week later, bands are fit on the molars, an impression is taken for the soldered appliance, and the patient is brought to the consultation room for the case presentation. At the same time as the case presentation, the assistant has already pre-bent the lower lingual holding arch from the study models and has poured the impression in quickset stone. Five minutes later the model is ready for soldering, and the pre-bent lingual holding arch is finished by the time the case presentation is completed. This allows us to insert the lower lingual holding arch immediately following the case presentation, and the patient has spent approximately 60 minutes in our office. This same protocol is also utilized for Hyrax expanders and space maintainers. Patients appreciate this type of efficiency, and on our posttreatment surveys, one of the most frequent words to describe our office is “efficient.”
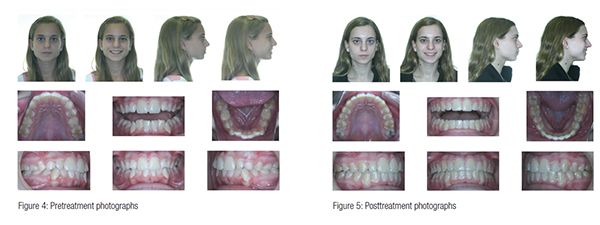
Due to the improvement in the lower incisors, this patient’s fixed-appliance treatment lasted 15 months, and she had 10 office visits during the fixed-appliance phase (Figures 4 and 5). This type of result is very predictable. Alleviating the lower crowding prior to placement of the fixed appliances shortens the time in braces, which leads to multiple efficiencies: fewer emergency appointments, better oral hygiene, increased profitability for the practice, and most importantly, happier patients.
Driftodontics and efficiency
“Driftodontics” is a term that can be attributed to Dr. R.G. “Wick” Alexander in his 1986 textbook2. He defines it as the late placement of orthodontic appliances after removal of permanent teeth. He notes that lower incisor crowding tends to unravel, and the premolars and canines drift distally into the extraction space. I have found driftodontics to be useful when adolescent patients present in the adult dentition, and they are borderline extraction cases. If extractions are indicated, the premolars are extracted, and patients return in 6 months. Most of the advantages of driftodontics have occurred in the first 6 months, and they are generally ready for placement of their braces. This strategy is most successful if there is minimal skeletal discrepancy and an average overbite.
 For example, this 11-year 3-month old female (Figure 6) presented with moderate maxillary and mandibular crowding, moderately procumbent incisors, and minimal overbite/overjet. Since she has advanced dental development relative to her chronological age, she is an ideal candidate for driftodontics since there are not as many social pressures to start treatment at age 11. Also, she has not yet entered her adolescent growth spurt, which has been shown to be the most efficient time to move teeth. Parents and patients easily understand that waiting 6 months without braces may shorten her time in braces by approximately 4 to 6 months. Everyone appreciates this strategy, and patients do not wish to spend any more time in braces than necessary.
For example, this 11-year 3-month old female (Figure 6) presented with moderate maxillary and mandibular crowding, moderately procumbent incisors, and minimal overbite/overjet. Since she has advanced dental development relative to her chronological age, she is an ideal candidate for driftodontics since there are not as many social pressures to start treatment at age 11. Also, she has not yet entered her adolescent growth spurt, which has been shown to be the most efficient time to move teeth. Parents and patients easily understand that waiting 6 months without braces may shorten her time in braces by approximately 4 to 6 months. Everyone appreciates this strategy, and patients do not wish to spend any more time in braces than necessary.
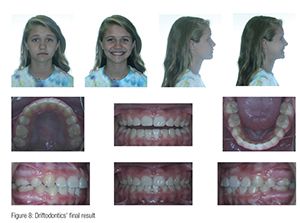 Six months following the extraction of her second premolars (Figure 7), the majority of her extraction space is closed, and the crowding has improved. Also, note the improved position of her canines and the slight deepening of her overbite. Her orthodontic appliances were placed, and she had a total of 11 visits over 14 months (Figure 8). She was treated with .022 Roth prescription twin brackets and finished with full-size stainless steel wires that were left in place for the final 2 months of treatment. Had she been treated with self-ligating braces, the manufacturer would be advertising, “a four-premolar extraction case treated in only 14 months!” The reality is that teeth do not know what type of brace is used, and the brace is only a handle to deliver a force system. Forces move teeth, not the highly marketed name-brand brackets and gadgets. Orthodontists are best able to manage these force systems, and there are a large number of excellent force systems on the market.
Six months following the extraction of her second premolars (Figure 7), the majority of her extraction space is closed, and the crowding has improved. Also, note the improved position of her canines and the slight deepening of her overbite. Her orthodontic appliances were placed, and she had a total of 11 visits over 14 months (Figure 8). She was treated with .022 Roth prescription twin brackets and finished with full-size stainless steel wires that were left in place for the final 2 months of treatment. Had she been treated with self-ligating braces, the manufacturer would be advertising, “a four-premolar extraction case treated in only 14 months!” The reality is that teeth do not know what type of brace is used, and the brace is only a handle to deliver a force system. Forces move teeth, not the highly marketed name-brand brackets and gadgets. Orthodontists are best able to manage these force systems, and there are a large number of excellent force systems on the market.
Serial extraction and efficiency
Despite the improvements in technology that allow for fewer patients to require extractions, there are always patients who have significant enough crowding to eventually require removal of premolars. This 9-year 9-month old female (Figure 9) presented with early loss of her primary canines, and retroclined mandibular incisors (IMA = 84.4).
Her space analysis indicated that even with extraction of four premolars, there would be minimal excess space. The other concern is that with extractions, the mandibular incisors may tip further lingual, causing a deepening of the bite and flattening of her profile. Therefore, a mandibular lingual holding arch was placed, and once the first premolars erupted, progress records were taken, and I decided to extract the four first premolars. When she presented 2½ years later, her crowding had been resolved, and there was no significant change in the overjet or overbite, and her mandibular incisor angulation had been maintained (Figure 10). Once the upper-left canine erupted, she was ready for her fixed appliances.
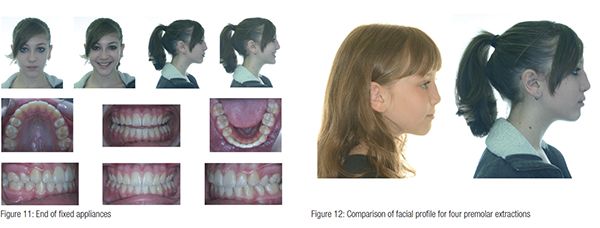
Her fixed-appliance therapy lasted 15 months, and she had 13 visits in our office (Figure 11). The key to achieving the shortest treatment time and fewest visits is to wait for all the teeth to erupt prior to placing appliances. Patients and parents understand that the goal is not to place the appliances; it is to remove the appliances in the shortest, most efficient time possible.
It is also important to note that many of the manufacturers promote “broad smiles and full lips” as a product of their non-extraction treatment. While I agree that lip position is influenced by tooth position, extraction treatment that is properly diagnosed and managed can result in full lips as was demonstrated by this patient (Figure 12).

Space maintenance and efficiency
Patients are often referred to an orthodontist due to early loss of primary teeth. The orthodontist must decide either to regain the space or to manage the lost space with the possibility of premolar extraction in the future. Some of our patients not only demand minimal time in braces, but also may request treatment with removable aligners. The following patient demonstrates that a Class II maxillary first-premolar extraction case can be managed with Invisalign express in only 5 months of aligners. This is the ultimate in efficient orthodontic treatment.

This 7-year 1 month-old female (Figure 13) was referred by her dentist due to early loss of her maxillary primary second molars, which had resulted in a Class II molar relationship. She was presented the following options: moving the maxillary first molars distal to create sufficient room for eruption of the second premolars, or utilizing a transpalatal arch to minimize further drift of the molars and re-evaluate for possible extraction of maxillary first premolars. After reviewing both options, the patient and her parents decided upon the transpalatal arch and re-evaluation in the future.
 At age 10, it was decided to extract the maxillary first premolars and re-evaluate for fixed appliances when she entered the adult dentition. In retrospect, this was the most efficient decision she could have made because the result was so good that it was not until age 15 that the patient decided she would like to finish her treatment (Figure 14).
At age 10, it was decided to extract the maxillary first premolars and re-evaluate for fixed appliances when she entered the adult dentition. In retrospect, this was the most efficient decision she could have made because the result was so good that it was not until age 15 that the patient decided she would like to finish her treatment (Figure 14).
Her request at this time was not to have braces at all and have treatment with Invisalign appliances to improve the alignment of her teeth. In fact, she was a candidate for Invisalign express and required only 10 aligners (Figure 15). With the advent of Invisalign, I am often finishing phase I treatment with the goal of being able to offer patients Invisalign for phase II if they request it. This has been an important change in phase I treatment planning.
Conclusion
Orthodontists often present efficiency to the public as a product only of high technology that is often expensive. The patients presented in this paper show that efficiency can be achieved with proper diagnosis and treatment planning that is not expensive and does not rely on “high technology” products. This type of efficiency is a product of education, experience, and honest treatment options. Some of these extraction patients could have been treated non-extraction, however they could not have been treated more efficiently with a more stable result. These are treatment options that should be presented to the patient.
If our profession is to survive, we must market ourselves to the public not as providers of technology, but as highly trained and educated orthodontists who provide excellent results for our patients in the shortest treatment time at a reasonable cost. If we present only technology, the manufacturers will market us as “providers” instead of orthodontists. We all know what has happened to our medical colleagues once insurance companies labeled them as “providers” instead of doctors. Patients are not loyal to providers since anyone can provide a service. Patients who receive excellent results in the shortest treatment time are very loyal to their orthodontists.
1. Brennan MM, Gianelly AA. The use of the lingual arch in the mixed dentition to resolve incisor crowding. Am J Orthod Dentofacial Orthop. 2000;117(1):81-85.
2. Alexander RG. The Alexander Discipline – Contemporary Concepts and Philosophies. Orange, CA: Ormco Corporation; 1986.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
