Dr. Robert Waugh discusses how an oral appliance can solve issues for patients with sleep apnea
The treatment of sleep apnea by orthodontists is a natural next step in the evolution of the specialty. My interest in the connection between the two began some years ago after attending courses on sleep medicine and realizing it was an emerging field that could help me become a better orthodontist. I later acquired a dental sleep practice from my mentor, Dr. Bob Ward, who also encouraged me to take my boards to become a Diplomate with the American Academy of Dental Sleep Medicine (AADSM). Reviewing my cases recently in preparation for the boards made me realize just how many patients had been treated for sleep apnea. Many had been referred by their GPs or physicians to have devices made for mild to moderate sleep apnea, which makes perfect sense. Orthodontists are already experts when it comes to fabricating appliances; when the conditions are right, and an oral appliance is made, we are often able to solve some problems for the patient that otherwise could be devastating (and most patients are grateful for a discreet sleep device rather than a loud, bulky CPAP machine).
Unlike my younger patients, sleep patients are patients for life. Common to orthodontics, I rarely see children and teens once their orthodontic treatment is complete, and am often left wondering how their lives have been impacted by my work. However, I’ve found that there can be a connection between both fields — dental sleep medicine and orthodontics — that makes me a better doctor for both my older and younger patients.
Case report
A 56-year-old male patient presented on the sleep medicine side of my practice. A scare with atrial fibrillation had caused him to more seriously seek treatment for his sleep apnea, which was making him wake up at night gasping for air, leading to increased blood pressure and putting him at risk for stroke. A skeletal deficiency of the lower jaw resulting in an overbite was observed, which caused his tongue to block his airway while sleeping. The patient had expected a sleep appliance or CPAP to fix the problem; however, with the position of his mandible, an orthognathic procedure to bring his jaw forward was suggested. Of course, like any surgery, it carried certain risks, and the patient wanted to be sure it was the best course of action.
A baseline CBCT scan was taken with the CS 9300 (Carestream Dental) with the patient in his normal bite to serve as a predictor of success for either a sleep appliance or surgery (Figure 1). Then, following the recommendations of a poster presentation from the the AADSM 2017 Annual Meeting, “CBCT in the Study of Different Phenotypes of Responders and Non-Responders of Mandibular Advance Device Treatment: A Preliminary Study,”1 a second low-dose scan was taken with the patient’s mandible postured forward 8 mm as it would be with either an appliance or after mandibular advancement (Figure 2). After two clicks — one to define the upper limit and one for the lower limit — the airway was automatically segmented using the CS Airway module (Carestream Dental) to highlight constrictions in the pharyngeal airway. The software, with its illustrative color-coding of the airway, served as a powerful communication tool with the patient. He was then more comfortable pursuing mandibular advancement over CPAP or an oral appliance and accepted treatment.
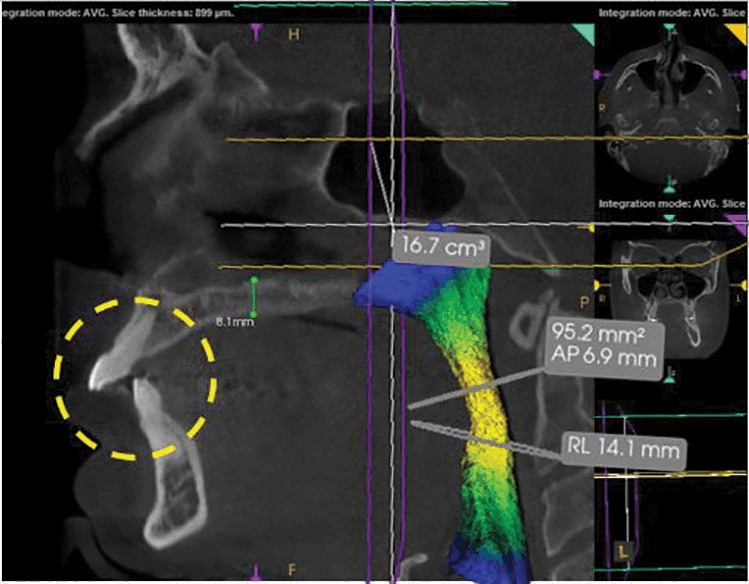
Figure 1: Maximum intercuspation
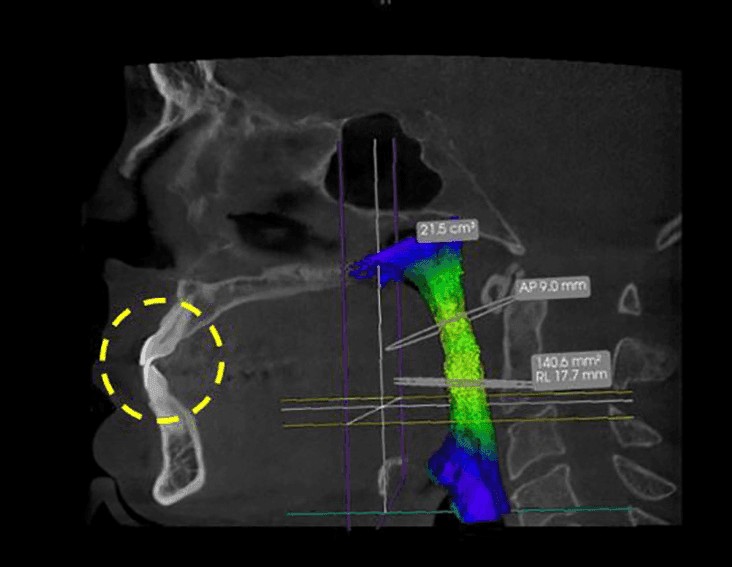
Figure 2: Protruded sagittal view
First, however, to compensate for the new position of the mandible, the patient opted for a micro-implant assisted maxillary skeletal expander (MSE), developed by Dr. Won Moon. This new style of TAD-based palatal expander is quickly gaining popularity, as it is less invasive for adults. The expander was custom-made to receive four screws — two on the left, two on the right — and stabilized by bicortical engagement. The existing CS 9300 CBCT scans were used for planning to ensure safe placement of the TADs (Figures 3-5).

Figure 3: Frontal view of TADs for MSE

Figure 4: Sagittal view of TADS for MSE
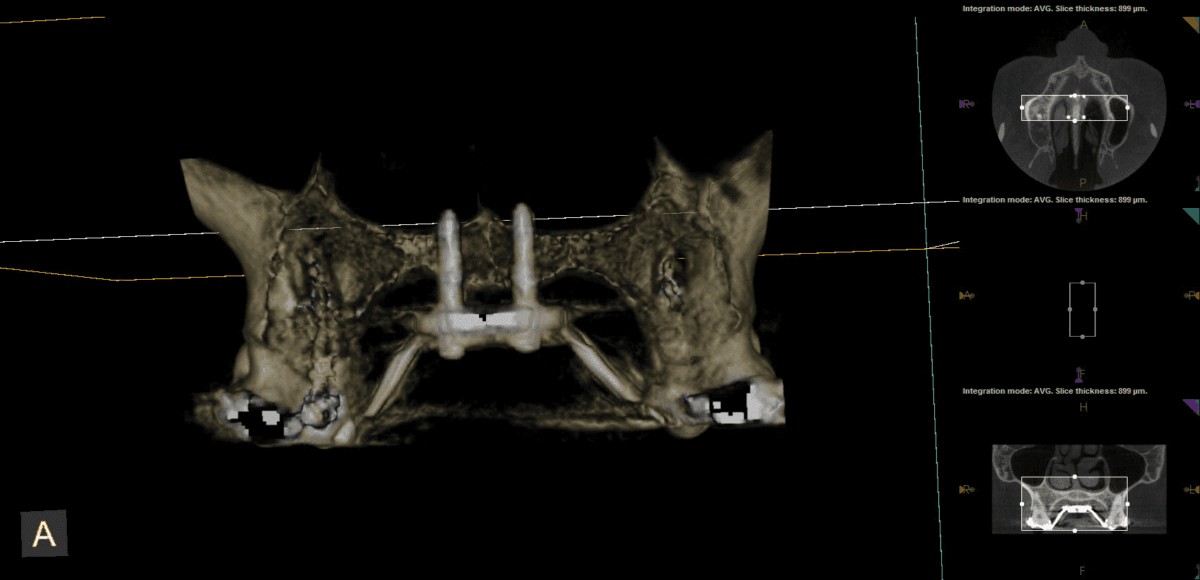
Figure 5: Surface volume for MSE
After maxillary expansion, next, the patient will receive braces, followed by orthognathic surgery approximately 1 year into treatment to advance the mandible. Treatment will be finalized with post-operative detailing.
Taking on sleep apnea cases such as these have made me a better clinician. I often find myself on the sleep medicine side of the practice consulting patients like this — in their 50s to 60s with a deficient lower jaw, struggling to breathe and with heart problems. Then I go to the orthodontic side of the practice to see a 7-year-old with a deficient mandible and need to decide between orthopedic treatment, extraction, or non-extraction — all of which have an impact on the tongue space. With the sleep apnea patient at the back of my mind, I may be encouraged to consider an orthopedic route with the orthodontic patient to give him/her a chance of unobstructed breathing for a lifetime.
 Robert Waugh, DMD, has practiced orthodontics full time in Athens, Georgia, since 1989 and is also an Assistant Professor at the Dental College of Georgia’s Orthodontic Residency program. Dr. Waugh’s interests include using new technologies that help deliver better care for his patients. In 2008, he merged three offices into one facility of 24 chairs that allows him to deliver care using a wide variety of advanced modalities in hygiene, patient scheduling, treatment delivery, and more. Dr. Waugh graduated from the Medical College of Georgia School of Dentistry in 1987 with both a DMD and a Masters in Oral Biology and was elected to Omicron Kappa Upsilon (OKU), the national dental honor society. He earned his orthodontic certification and a second Master’s degree at Baylor University in 1989. In 2000, he was board-certified by the American Board of Orthodontics. Dr. Waugh has served as President of the Georgia Association of Orthodontists and is a member of the International and American Colleges of Dentists.
Robert Waugh, DMD, has practiced orthodontics full time in Athens, Georgia, since 1989 and is also an Assistant Professor at the Dental College of Georgia’s Orthodontic Residency program. Dr. Waugh’s interests include using new technologies that help deliver better care for his patients. In 2008, he merged three offices into one facility of 24 chairs that allows him to deliver care using a wide variety of advanced modalities in hygiene, patient scheduling, treatment delivery, and more. Dr. Waugh graduated from the Medical College of Georgia School of Dentistry in 1987 with both a DMD and a Masters in Oral Biology and was elected to Omicron Kappa Upsilon (OKU), the national dental honor society. He earned his orthodontic certification and a second Master’s degree at Baylor University in 1989. In 2000, he was board-certified by the American Board of Orthodontics. Dr. Waugh has served as President of the Georgia Association of Orthodontists and is a member of the International and American Colleges of Dentists.
Disclosure: Dr. Robert Waugh is a key opinion leader for Carestream Dental.
- Mayoral Sanz P, Contreras MM, Domínguez-Mompell R. CBCT in the study of different phenotypes of responders and non-responders of mandibular advance device treatment: a preliminary study. Poster presented at: 26th Annual Meeting of the American Academy of Dental Sleep Medicine; June 2-4, 2017; Boston, MA.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
