Editor’s intro: Dr. Antonino Secchi illustrates how orthodontists are improving smiles and also impacting self esteem.
Dr. Antonino Secchi illustrates his two-phase treatment plan
A few years ago I had the opportunity to treat a little girl with a rather big self-confidence problem mainly due to her smile. We always praise our specialty for changing people’s lives as we improve their smile and self-confidence, but it takes a case like Caitlin’s to really appreciate the power of what we do with orthodontics, and how much we can positively affect someone’s personality and self-esteem.
Caitlin, an 11-year-old female, consulted in our office with the chief complaint of “my front tooth is sticking out of my mouth.” Her medical history was not relevant, and she had no dental and/or TMJ pain or discomfort. She was in late mixed dentition, showing Class II end-on with severe crowding on her upper arch and moderate crowding in her lower arch. Her upper right central incisor was ectopically positioned (Figure 1). She had a skeletal transverse discrepancy diagnosed using the CAC analysis.1-3 Her maxilla was narrow when compared to her mandible.

My treatment plan was to treat Caitlin in two phases:
- Phase 1 with a rapid palatal expander (RPE) to correct the transverse dis-crepancy in conjunction with partial bonding of the upper arch to improve the alignment, specifically of the upper right central incisor.
- Phase 2 with comprehensive ortho-dontic treatment bonding the upper and lower arch
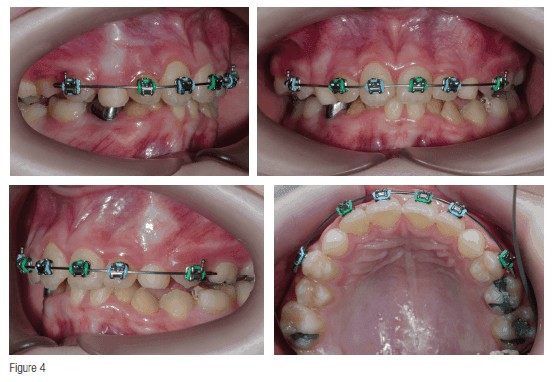
Phase 1 treatment (Figures 2-4)
 A Haas-type RPE was cemented and activated at a rate of two turns per day for 20 days to open the expander 10 mm. Once the RPE activation was finished, we partially bonded the upper arch, including first pre-molars, lateral incisors, and central incisors. The appliance used was an In-Ovation® R CCO® (Complete Clinical Orthodontics) Rx (Dentsply Sirona Orthodontics). The initial wire was a 0.014″ Sentalloy® followed by a 0.020″ x 0.020″ BioForce® (Sentalloy and BioForce are thermal activated superelastic wires from Dentsply Sirona Orthodontics). The RPE was removed after 4.5 months. The 0.014″ Sentalloy and the 0.020″ x 0.020″ BioForce were in place for 4 months each. This phase of treatment lasted a little over 8 months. The main two objectives, to correct the transverse discrepancy and to align the maxillary incisors, were achieved.
A Haas-type RPE was cemented and activated at a rate of two turns per day for 20 days to open the expander 10 mm. Once the RPE activation was finished, we partially bonded the upper arch, including first pre-molars, lateral incisors, and central incisors. The appliance used was an In-Ovation® R CCO® (Complete Clinical Orthodontics) Rx (Dentsply Sirona Orthodontics). The initial wire was a 0.014″ Sentalloy® followed by a 0.020″ x 0.020″ BioForce® (Sentalloy and BioForce are thermal activated superelastic wires from Dentsply Sirona Orthodontics). The RPE was removed after 4.5 months. The 0.014″ Sentalloy and the 0.020″ x 0.020″ BioForce were in place for 4 months each. This phase of treatment lasted a little over 8 months. The main two objectives, to correct the transverse discrepancy and to align the maxillary incisors, were achieved.
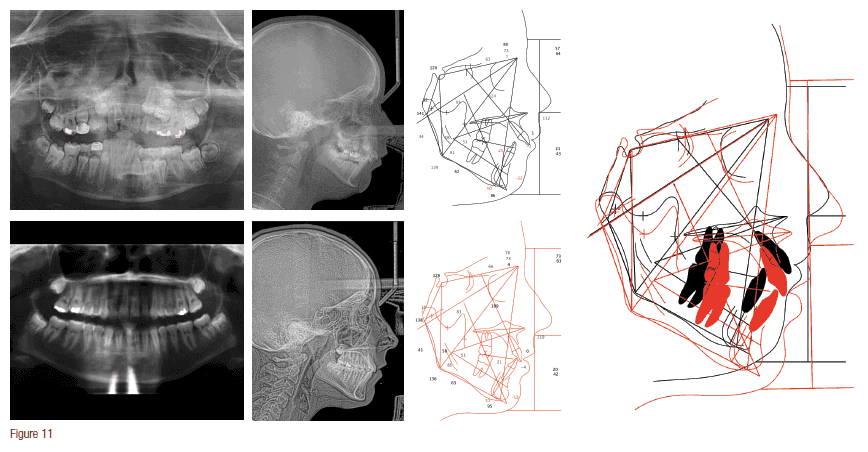
Phase 2 treatment (Figures 5-11)
Needless to say, after Phase 1, Caitlin and her mother were very happy with the result. They were excited and anxious to start “full braces” and, therefore, we decided to start Phase 2 a little earlier than what I would have wanted since the upper canines were not in yet. They understood that starting now would probably make the overall treatment time longer, but they were fine with that.

For full bonding of the upper and lower arch, we used In-Ovation R CCO Rx. This phase of treatment was divided in three stages following the CCO treatment mechanic sequence.4-6 For Stage 1 (Figure 5), we used a 0.014″ Sentalloy followed by a 0.020″ x 0.020″ BioForce wire with the objective of leveling, aligning, correcting all rotations, and beginning to level the occlusal plane. For Stage 2 (Figures 6 and 7), we used a 0.019″ x 0.025″ SS wire. At this stage, upper and lower wires were co-ordinated to achieve the proper overjet from molar to molar. Spaces were consolidated using a power chain. The occlusal plane was completely leveled thanks to the stiffness of the steel wires, and sagittal correction was achieved using short Class II elastics (3/16″ 4 oz) from upper canine to lower second premolar.
For Stage 3 (Figure 8), we used a braided 0.019″ x 0.025″ SS wire. Although this wire is a steel wire since it is braided, it provides enough flexibility to be able to improve the intercuspation when using elastics in a vertical triangular fashion (3/16″ 4 oz). Also, if there is the need to do any bracket reposition, this wire can easily engage the bracket from it new position.

After 24 months, braces were removed, teeth were polished, and upper and lower Essix retainers were given to Caitlin with the instruction of wearing them every day at nighttime.
Orthodontically speaking, most goals were achieved, and Caitlin’s smile was greatly improved (Figures 9-11). However, the changes between the before-and-after treatment pictures cannot properly show how much Caitlin’s confidence, self-esteem, and overall happiness were transformed. In our daily busy schedule, when sometimes treatments fall into a routine, it is good to be reminded that often we do a lot more than straighten teeth.

Editor’s call to action
Impacting self esteem through orthodontics doesn’t have to take a lot of time. Read about Dr. Secchi’s cosmetic solution that took 15 weeks to achieve. https://orthopracticeus.com/case-studies/orthodontic-treatment-with-suresmile-aligners.
 Antonino G. Secchi, DMD, MS, is an alumnus of the University of Pennsylvania School of Dental Medicine, where he received his Doctorate of Dental Medicine, Certificate in orthodontics, and a Master of Science in oral biology. Dr. Secchi is a Diplomate of the American Board of Orthodontics and a member of the prestigious Edward H. Angle Society of Orthodontists. He also holds membership in various local, national, and international dental and orthodontic societies and was the 2016 President of the Greater Philadelphia Society of Orthodontists. He is currently in practice in Pennsylvania.
Antonino G. Secchi, DMD, MS, is an alumnus of the University of Pennsylvania School of Dental Medicine, where he received his Doctorate of Dental Medicine, Certificate in orthodontics, and a Master of Science in oral biology. Dr. Secchi is a Diplomate of the American Board of Orthodontics and a member of the prestigious Edward H. Angle Society of Orthodontists. He also holds membership in various local, national, and international dental and orthodontic societies and was the 2016 President of the Greater Philadelphia Society of Orthodontists. He is currently in practice in Pennsylvania.
Disclosure: Dr. Secchi is the founder of the Complete Clinical Orthodontics System™ (CCO System), which he teaches to orthodontists in the United States and worldwide.
- Hayes JL. In search of improved skeletal transverse diagnosis. Part 1. Orthodontic Practice US. 2010;1(3):34-39.
- Hayes JL. In search of improved skeletal transverse diagnosis. Part 2: A new measurement technique used on 114 consecutive untreated patients. Orthodontic Practice US. 2010;1(4):34-39.
- Hayes JL. Proposed clinical skeletal transverse measurement technique—palpation adjacent to the molars. Orthodontic Practice US. 2011;2(2):28-29.
- Secchi AG. Complete Clinical Orthodontics: Treatment Mechanics Part 1. Orthodontic Practice US. 2013;4(1): 28-35.
- Secchi AG. Complete Clinical Orthodontics: Treatment Mechanics Part 2. Orthodontic Practice US. 2013;4(2): 28-32.
- Secchi AG. Complete Clinical Orthodontics: Treatment Mechanics Part 3. Orthodontic Practice US. 2013;4(3): 38-41.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
