Dr. Ana Maria Cantor discusses treatment for a patient’s esthetic challenge
Class III malocclusions are classified into four types of skeletal and dental relationships with either 1) mandibular protrusion, 2) maxillary retrusion, 3) a combination of the two, or 4) a normal relationship of the jaws.1–3 The prevalence of Class III mal-occlusions is estimated to be 1% to 10%, depending on ethnicity, sex and age. The etiology may be skeletal or dentoalveolar.4 The incidence of lateral incisor agenesis in the permanent dentition is estimated to be between 1.6% and 9.6%,5,6 and there is a correlation between the size of the maxilla and agenesis of maxillary teeth.6
The two possible therapeutic options for adult patients with Class III malocclusions are orthognathic surgery or camouflage orthodontics.7 Regardless of the option chosen, it is important to take into consideration increasing the angle of convexity (ANB) to improve the profile of the face with a greater increase in the length of the upper lip.8 It is, however, often difficult to predict the result that can be offset by labial inclination of the maxillary incisors and the subsequent negative effect on the patient’s smile,9 as well as retro-inclination of the mandibular incisors, with deleterious effects on the periodontium.
The combination of Class III malocclusion with missing maxillary lateral incisors can be challenging to resolve satisfactorily while enhancing the facial profile of the patient given the constriction of the maxilla. In patients with these characteristics, a combination of orthognathic surgery and orthodontics with a bridge or implants is often recommended.10 Given that the patient in the following case report would not consider orthognathic surgery or opening space orthodontically for the placement of implants, the alternative recommended was camouflage orthodontic treatment. The case report is intended to illustrate treatment of a Class III malocclusion exhibiting maxillary lateral incisor agenesis with the use a simple Class III functional appliance for anterior-posterior correction, followed by fixed self-ligating appliance therapy.
Diagnosis and treatment plan
A 30-year-old female patient presented with a concave profile and maxillary hypoplasia with a short upper lip and lower retracted labial protrusion, an obtuse nasolabial angle, and skeletal Class III maxillary retrusion and mandibular protrusion. Dentally, the patient exhibited a Class III malocclusion with marked crowding, an anterior crossbite, a 1 mm midline deviation, a moderate curve of Spee, and agenesis of the maxillary lateral incisors that the panoramic radiograph confirmed (Figures 1A–1J; Table 1).

Figures 1A-1J: Patient with a Class III malocclusion and agenesis of the maxillary lateral incisors before treatment
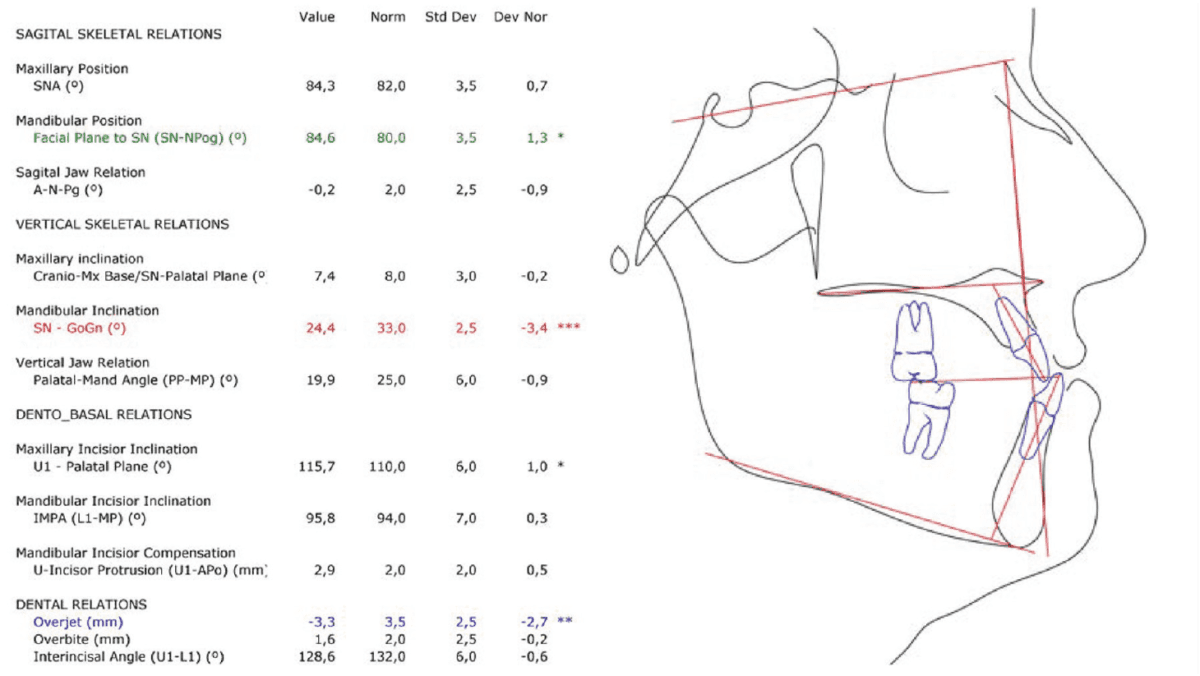
Table 1: Pretreatment cephalometric data
The treatment goals were to improve the patient’s facial esthetics, correct the Class III malocclusion exclusively with orthodontics, reduce the concavity of her profile, and create greater fullness of the upper lip, correct the anterior crossbite, distalize the mandibular posterior segment, protract the maxilla, and close the spaces from the congenitally missing lateral incisors, reconstructing the canines as lateral incisors and the first premolars as canines. Since the patient rejected the more invasive options recommended and opted for camouflage orthodontics, she was cautioned that a satisfactory result depended on her strict compliance with the treatment protocols, specifically the use of elastics.
Wire sequence
Treatment followed the Carriere® System (Henry Schein® Orthodontics) archwire sequence; except in this case the first wire was a 0.016 in. dimension wire rather than a 0.014 in. wire. The archwires were all thermally activated wires, with lower transformation temperatures chosen as archwire sizes increased to limit force on the periodontium:
• 0.016 in. Cu Nitanium (27°C)
• 0.014 × 0.025 in. Cu Nitanium (27°C)
• 0.017 × 0.025 in. Cu Nitanium (35°C)
• 0.019 × 0.025 in. Cu Nitanium (35°C).
Treatment progress
Treatment commenced with the simultaneous use of a Carriere® Motion 3D™ Class III Appliance (Henry Schein Orthodontics) for sagittal correction and Carriere® SLX™ (Henry Schein Orthodontics) 0.022 in. MBT prescription pre-adjusted, passive self-ligating brackets bonded with 0.016 in. Cu™ Nitanium® archwires (Henry Schein Orthodontics) engaged in the upper arch for anchorage. The Motion 3D Class III appliance was bonded directly to the mandibular canines and first molars with 6 oz, 0.25 in. intraoral elastics engaged for Class III traction to maxillary second molar tubes. Upper arch levelling and alignment was performed with 0.016 in. Cu Nitanium archwire, and bilateral stops placed mesially to the bonded first molar buccal tubes to assist with protraction of the upper arch.
Proper patient compliance achieved correct intercuspation in 4 months; the negative overjet had corrected to an end-on position in 5 months (Figures 2A–2C). At that point, the Motion appliance was debonded, and Carriere SLX 0.022 in. MBT prescription pre-adjusted, passive self-ligating brackets were bonded in the lower arch (Figures 3A–3C).

Figures 2A-2C: After 5 months of sagittal treatment, the negative overjet had corrected to an end-on position. Mild extrusion of the mandibular canine can be observed, which was expected and a positive sign of the effects of the sagittal correction. The result was an anticlockwise rotation of the posterior occlusal plane, producing significant improvement in the prognathic profile

Figures 3A-3C: After bonding the mandibular brackets
Treatment results
After 16 months, treatment concluded with the patient showing a significant profile improvement, a correction of the maxillary hypoplasia, anterior crossbite, and Class III malocclusion with greater upper lip fullness, a balanced smile line, adequate gingival margins, levelling, and suitable overjet and overbite. By replacing the congenitally missing lateral incisors with reconstructed canines and positioning reconstructed first premolars as canines, good occlusion was achieved (Figures 4A-4C).

Figures 4A-4C: After 14 months of treatment, the case demonstrated a corrected overjet, overbite, and intercuspation. The canines occupied the positions of the congenitally missing lateral incisors
For the re-anatomization of the canines and first pre-molars, we performed a laser diode gingivoplasty, then shaved the cusp tips of the canines and sculptured their distal and mesial borders with composite resin. Finally, we shaved and recontoured the palatal cusps of the first premolars to avoid premature contact at functional occlusion (Figures 5A–5J; Table 2).

Figures 5A-5J: Final photographs and radiographs of the patient after 16 months of treatment
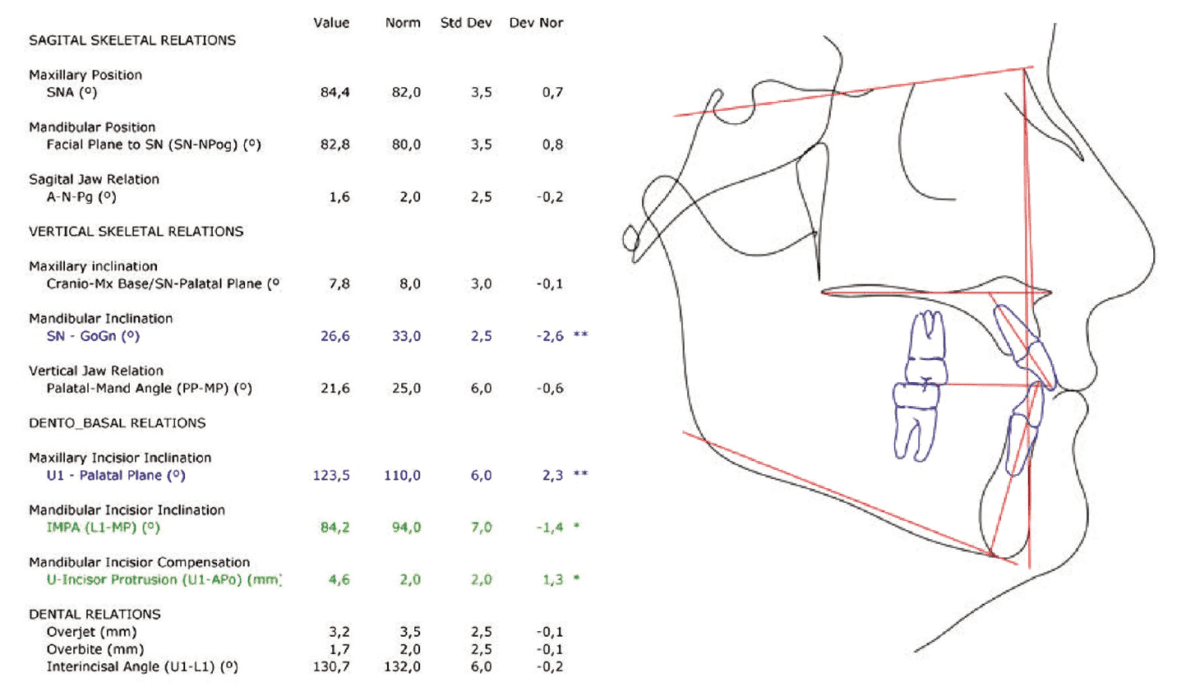
Table 2: Posttreatment cephalometric data
Discussion
Many Class III patients elect not to undergo invasive treatment that involves surgery, extractions, and/or implants, especially if treatment affects maxillary anterior teeth considered critical to overall smile esthetics. When such esthetic problems are presented, it is important that orthodontists have adequate training in and experience and awareness of facial esthetics to be able to offer more conservative solutions because such issues, if unresolved satisfactorily, can detrimentally affect the patients’ emotional state and self-esteem.
The position of the maxillary and mandibular incisors determines facial harmony and a pleasing smile. Maxillary lateral incisor agenesis makes obtaining good treatment results a challenge, especially with reduced maxillary arch length, owing to the lack of these important teeth.
Treatment plans for cases of maxillary hypoplasia with agenesis of the lateral incisors often call for opening space for implants. The greatest problem with such plans is that it is impossible to predict when, to what degree, or in which patients unattractive soft- and/or hard-tissue changes around implant-supported porcelain crowns, especially noticeable in the maxillary anterior teeth, will occur. Biological and technical complications are frequent and can appear even after only a few years.12
Space closure with protraction of the maxilla and later re-anatomization of the canines to replace the congenitally missing lateral incisors can be a good alternative. Handled carefully, this option avoids gingival retraction that can accompany implant placement or metal show-through on crowns, bridges, and implants that can occur in some restorations after a period. Clinicians treating Class III patients with maxillary hypoplasia have traditionally avoided space closure because of the potentially adverse effects on the profile. The combined use of the Carriere Motion 3D Class III Appliance and SLX Brackets for applicable cases biomechanically eliminates these side effects by optimizing the relationship between the maxilla and the mandible, both occlusally and esthetically,11 for better results than simply neutralizing the potentially adverse effects of opening space for implants.
Camouflage orthodontic treatment can result in protrusion8 of the maxillary incisors (giving an appearance of a short upper lip), as well as retro-inclination of the mandibular incisors, with deleterious effects on the periodontium. The actions of the Carriere Motion 3D Class III Appliance is distalization of the mandibular segments from molar to canine as a unit, with intrusion of the mandibular molars, extrusion of the mandibular canines, and retraction of the mandibular incisors — the result of which is an anticlockwise rotation of the posterior occlusal plane, producing a significant improvement in the prognathic profile.11 In Class III cases, choosing brackets rather than an aligner for anchorage and bonding them simultaneously with the functional appliance produces distalization of the mandibular posterior segment while achieving torque control of the maxillary incisors11 and space closure, yet with a protractor effect on the maxilla that develops upper lip fullness.

Figure 6: Superimposition of cephalometric tracings pre- and posttreatment

Figures 7A-7H: Photographs of the patient 3 years posttreatment
Conclusion
Treatment with the Carriere Motion 3D Class III Appliance is efficient for the correction of adult Class III malocclusions, producing satisfactory results both esthetically and functionally. The Carriere Motion 3D Class III Appliance used in combination with Carriere SLX Self-ligating Brackets is a biomechanically efficient means of addressing cases with maxillary hypoplasia. Compared with alternatives, such as a combination of surgery and conventional orthodontics for opening space for implants or bridges, these appliances can significantly reduce treatment time for treatment of Class III patients. In cases of agenesis of the maxillary lateral incisors, the approach represented by this case is an efficient alternative for closing spaces while balancing the patent’s profile and correcting the Class III malocclusion.
This article was previously published in Dental Tribune UK Ortho International. 2018;3(1):14-19.
 Dr. Ana Maria Cantor practices orthodontics at the private OdontoKids clinic in Malaga, Spain. She can be contacted at anamacantor@yahoo.es.
Dr. Ana Maria Cantor practices orthodontics at the private OdontoKids clinic in Malaga, Spain. She can be contacted at anamacantor@yahoo.es.
Disclosure: Dr. Cantor is a key opinion leader and paid speaker for Henry Schein Orthodontics.
- Sanborn, RT. Differences between the facial skeletal patterns of Class III malocclusion and normal occlusion. Angle Orthod. 1955;25(4):208-222.
- Jacobson A, Evans WG, Preston CB, Sadowsky PL. Mandibular prognathism. Am J Orthod. 1974;66(2):140-171.
- Ellise E 3rd, McNamara JA Jr. Components of adult Class III malocclusion. J Oral Maxillofac Surg. 1984;42(5):295-305.
- Staudt C, Kiliaridis S. Different skeletal types underlying Class III malocclusion in a random population. Am J Orthod. 1984;136(5):715-721.
- Boj JR, Catala M, Garcia-Ballesta C., Mendoza A. Abnormalities of dentition in pediatric dentistry: The evolvement of the boy to a young adult. 1st ed. Madrid: Ripano Ed.; 2011.
- Tavajohi-Kermani H, Kapur R, Sciote J. Tooth agenesis and craniofacial morphology in an orthodontic population. Am J Orthod Dentofacial Orthop. 2002;122(1):39-47.
- Proffit WR, Sarver D. Combined surgical and orthodontic treatment, in Contemporary Orthodontics. 4th ed. W.R. Proffit, H.W. Fields, Jr., D.A. Sarver, St. Louis, MO: Mosby; 2007.
- Burns NR, Musich DR, Martin C, Razmus T, Gunel E, Ngan P. Class III camouflage treatment: what are the limits? Am J Orthod Dentofacial Orthop. 2010;137:(1)9-11.
- Troy BA, Shanker S, Fields HW, Vig K, Johnston W. Comparison of incisor inclination in patients with Class III malocclusion treated with orthodontic surgery or camouflage. Am J Orthod Dentofacial Orthop. 2009;135:(2)146-147.
- Cozzani M, Lombardo L, Gracco A. Class III malocclusion with missing maxillary lateral incisors. Am J Orthod Dentofacial Orthop. 2011;139(3):388-396.
- Carriére L. Nonsurgical correction of severe skeletal Class III malocclusion. J Clin Orthod. 2016;50(4):216-23.
- Zachrisson BU, Rosa M, Toreskog S. Congenitally missing maxillary lateral incisors: canine substitution. Am J Orthod Dentofacial Orthop. 2011;139(4):434, 436, 438.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
