Editor’s intro: The primary treatment plan is not the only option. Read about how Dr. Michael Bicknell found an alternate way to achieve a successful treatment outcome.
Dr. Michael Bicknell discusses how two patients who declined the primary treatment plan still achieved an excellent outcome
Introduction
In today’s market, patients are exposed to numerous options when it comes to orthodontic care. In order to remain the clear and best option, the orthodontic specialist must be able to provide better outcomes and an improved patient experience to remain the provider of choice. Luckily, there has been amazing product innovation that we can use as tools in this endeavor. By coupling these innovative technologies with a desire for continual learning and refining of our skills, we can simplify our processes, reduce treatment times, and improve the patient’s experience — all while achieving excellence in our results. Exceptional patient results along with amazing patient experiences are what will continue to differentiate the orthodontic specialists from other market choices available, now and in the future.
When I began my clinical career, I was fortunate to have been taught by a wonderful group of instructors all with varying techniques. With today’s access to information, we are not only able, but also obligated to pursue improved techniques to deliver the highest quality of patient care. When I began using passive self-ligation (PSL), I was drawn to the beautiful smiles and artistry that I wasn’t seeing in my own cases. These amazing results were the primary reason for my move to PSL. It wasn’t until later that I realized, in addition to the beautiful smiles, PSL would also allow for increased efficiency, decreased sensitivity, and an improved patient experience.
There are times as orthodontists that we have an ideal treatment plan worked out, but it is not accepted by the patients or parents of our patients for a variety of reasons. This results in stress because of altering our recommendation to satisfy the patients’ requests and the fear of not being successful in our desired outcomes. The following two cases illustrate a deviation from the original treatment plan proposed due to strong patient objections over the recommended treatment. They also demonstrate the power of light forces, anterior torque control, and transverse dental development in regard to the treatment of crowding and Class II correction. The final results satisfied the original treatment objectives, provided excellent outcomes, and created very happy patients.
Case 1
Diagnosis
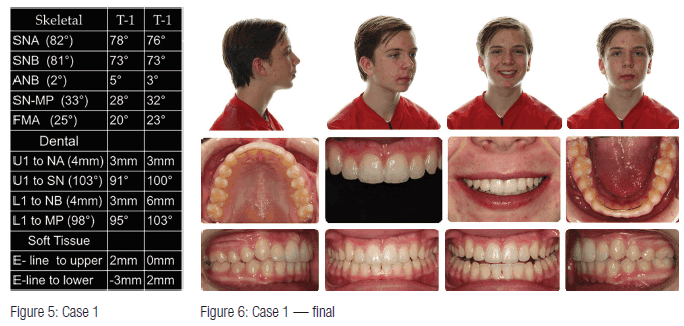
An 11½-year-old male presented with a Class II Division 1 malocclusion with severe maxillary crowding and moderate mandibular crowding. The facial profile was convex with a retrusive mandible. Thin lip strictures were noted along with tapered buccal segments and a poor smile arc due to insufficient incisor display when smiling.


Objectives/plan
The objectives were to create space for the U3’s while maintaining maxillary incisor position, attain Class 1 molars and canines, improve the smile arc by erupting incisors, and develop the posterior segments for increased arch length as well as improved smile width. The initial treatment plan presented included using a Herbst appliance to address the Class II malocclusion; however, the parent declined using the function appliance due to a strong bias against it. Therefore, passive self-ligation with Class II elastics was the treatment plan that was presented and accepted.
Case setup
The brackets chosen were Damon™ Q passive self-ligation standard torque upper and lower. The severe crowding in the maxillary arch would normally lead to a low torque bracket selection; however, the Class II elastics would negate the forward movement, thus the reason for the choice of standard torque. All permanent teeth were bonded except for the U3’s. The U/L 5’s along with the U/L 7’s would be bonded once they erupted. As an observation, initiating treatment while the deciduous second molars are present helps with the Class II correction by utilizing the e-space, assuming the patient is wearing Class II elastics when they are exfoliated. The bite was disarticulated, and 2 oz. 3/16 elastics were started from the U4’s to the L6’s.
Case progression
Visit 1: Bracket placement with 0.014 CuNiTi U/L and NiTi open coil springs from the U2-U4 R/L were placed to create space for the U3’s. An early elastic protocol was started using 2 oz. 3/16 Class II elastics from the U4’s to the L6’s full-time. The occlusion was disarticulated by placing bite stops on the U6’s to reduce the effects of incline planes. The next appointment interval was 10 weeks.
Visit 2: Change wires to 0.018 CuNiTi U/L with activation of open coil springs and continue Class II elastics. The next appointment interval was 10 weeks.
Visit 3: Change wires to 0.14 x 0.025 CuNiTi U/L with activation of open coil springs and continue Class II elastics. The next appointment interval was 10 weeks.
Visit 4: Maintain archwires with activation of open coil springs and allow U3’s to erupt. The next appointment interval was 10 weeks.
Visit 5: Bond U3’s, replace wires, and continue Class II elastics. The next appointment interval was 8 weeks.
Visit 6: Change wires to 0.018 x 0.025 CuNiTi U/L and continue Class II elastics. The next appointment interval was 8 weeks.
Visit 7: Progress records were taken, and repositioning of brackets was completed along with bonding of the U/L 5’s. Archwires were changed to 0.014 x 0.025 CuNiTi U/L due to the position of 5’s. The next appointment interval was 8 weeks.
Visit 8: Change wires to 0.18 x 0.025 CuNiTi U/L, and continue Class II elastics. The next appointment interval was 8 weeks.
Visit 9: Change wires to 0.019 x 0.025 stainless steel (SS) upper and 0.016 x 0.025 SS lower, Lace U3-3 and place tiebacks from posts to U6’s on the upper arch. The next appointment interval was 6 weeks.
Visits 10-12: Finishing details were completed along with direct placement of the upper 2112 braided SS fixed retainer and a digital scan for interim U/L Essix retainers and a custom-made 0.026 SS fixed L3-3.
Posttreatment follow-up: Final records and scan for final Essix retainers — two sets U/L worn at night.

Overview
An overview of the case resulted in the Damon Q passive self-ligation standard torque upper and lower correcting the Class II maloccluision to functional Class I occlusion along with substantial arch development. Maxillary incisor position and angulation were maintained with some advancement and proclination of the lower incisors observed. Overall, the patient grew in a favorable direction and was very compliant, only requiring 2oz. 3/16 elastics for the duration of the treatment worn from the U4’s to the L6’s. From a clinical efficiency standpoint, the patient had 12 treatment visits and was completed in 18 months.
Case 2
Diagnosis
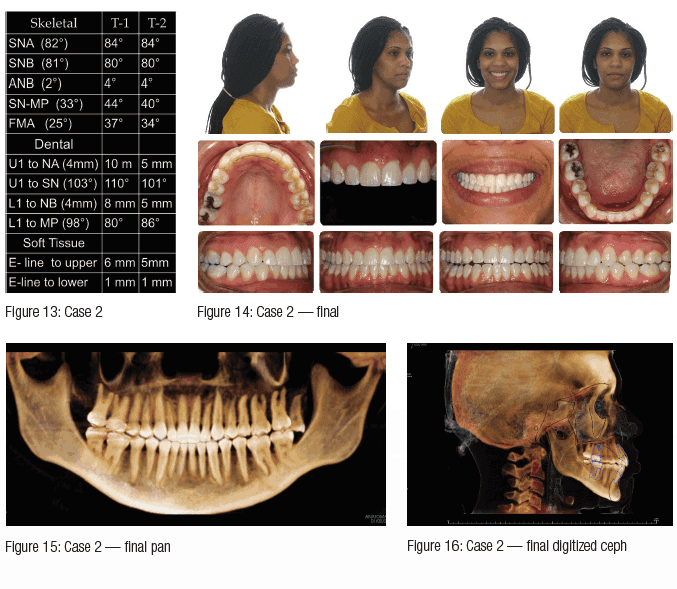
A 28-year-old female presented with a Class II Division 1 malocclusion with moderate maxillary crowding and mild mandibular crowding. The mandibular first molars were missing due to previous extractions as a child, resulting in mesial tipping of the second molars. Over-eruption of the maxillary left first molar was evident from the effects of the extractions as well. The facial profile was convex with a well-positioned mandible. Radiographic analysis shows protruded and proclined maxillary incisors and protruded lower incisors. Lips were full and protruded along with tapered buccal segments and a poor smile arc due to insufficient incisor display when smiling.

Objectives/plan
The objectives were to improve maxillary incisor position through retraction, attain Class I canines, improve the smile arc by erupting incisors, and develop the posterior segments for improved smile width. The initial treatment plan presented included extraction of U4’s to reduce overjet and retract incisors; however, the patient had such a negative experience as a child with the removal of the mandibular first molars that she would not allow additional extractions. Therefore, a non-extraction plan using passive self-ligation with Class II elastics, along with the use of temporary anchor devices (TADs) to protract the mandibular posterior segments and to intrude the maxillary left first molar, was the treatment plan that was accepted.
Case setup
The brackets chosen were Damon Q passive self-ligation standard torque upper and lower with high-torque brackets on the maxillary canines. All permanent teeth were bonded, and four 8mm VectorTAS™ were placed — one on the buccal and one on the palatal of the UL6 to intrude, and one between the mandibular canine and first premolar on both the right and left sides. A stainless steel ligature tie was twisted and ligated from the TAD to the first molar bracket to prevent distal movement of the crown and to encourage mesial root tip of the first molars during leveling. The bite was disarticulated, and 2 oz. 3/16 elastics were started from the U4’s to the L6’s.
Case progression
Visit 1: Bracket placement with initial 0.014 CuNiTi U/L and placement of TADs as noted above. An early elastic protocol was started using 2 oz. 3/16 Class II elastics from the U4’s to the L6’s full-time. The occlusion with disarticulation by placing bite stops on the U6’s to reduce the effect of incline planes. The next appointment interval was 10 weeks.
Visit 2: Change wires to 0.018 CuNiTi U/L. Activate intrusion on the UL6. The next appointment interval was 10 weeks.
Visit 3: Change wires to 0.14 x 0.025 CuNiTi U/L. Activate intrusion on the UL6. The next appointment interval was 10 weeks.
Visits 4-6: Change wires to 0.018 x 0.025 CuNiTi U/L, and continue Class II elastics. At this point, the UL6 was level, and the intrusion was complete; therefore, the maxillary TADs were removed. The mandibular first molars were still uprighting, so the current wires were maintained for three visits, and the patient was seen every 10 weeks. Uprighting was complete, and the mandibular TADs were removed at the sixth visit, which was 60 weeks into treatment.
Visit 7: Progress records were taken, repositioning of brackets was completed, and the archwires were maintained for an additional 4 weeks.
Visit 8: Change wires to 0.019 x 0.025 SS upper and 0.016 x 0.025 SS lower, lace U3-3, and place tiebacks from posts to U6’s on the upper arch. The next appointment interval was 6 weeks.
Visits 9-13: Finishing details along with esthetic gingival recontouring was completed on the U2-2. Retention plan included direct placement of the upper 2112 braided SS fixed retainer and a digital scan for interim U/L Essix retainers with a custom-made 0.026 SS fixed L3-3.
Posttreatment follow-up: Final records and scan for final Essix retainers — two sets U/L worn at night and a referral was given for removal of the maxillary left third molar.
Overview
An overview of the case resulted in the Damon Q PSL standard torque upper and lower correcting the Class II malocclusion to a functional Class I occlusion along with substantial arch development. Maxillary incisor position was improved, and angulation was maintained. The significant arch development created along with the Class II elastics allowed for the incisor retraction. The patient was very compliant, only requiring 2 oz. 3/16 elastics for the duration of the treatment worn from the U4’s to the L6’s. From a clinical efficiency standpoint, the patient had 13 treatment visits and was completed in 23 months.
Summary and conclusion
The two case examples presented illustrate many of the outcomes that become very predictable with the Damon System. Significant transverse arch development, Class II correction using light elastics, and torque control of the incisors are only a few of the benefits that help improve our clinical results. Shorter treatment times, reduced number of appointments, and decreased discomfort provide an improved patient experience. With the newest addition to the Damon System, the Damon Q2 bracket —featuring 2x rotational control for improved precision, predictability, and reliability —treatment efficiency can be increased. Because of this, I have incorporated Damon Q2 into all of my treatment cases. In an ever-changing market filled with multiple choices by our patients, providing excellent results along with enhanced patient experience will differentiate the orthodontic specialist as the best choice for orthodontic treatment to our patients.
Editor’s call to action
Whether it’s for your primary treatment plan or an alternative, read more about how the Damon™ Q2 offers optimal rotation control. https://orthopracticeus.com/product-profile/damon-q2
 Michael Bicknell, DDS, MS, earned his DDS and completed a residency in orthodontics at the University of Illinois at Chicago College of Dentistry where he also received a MS in oral biology. He is a former clinical instructor at the university and continues his involvement there by lecturing to dental students and orthodontic residents throughout the year. In private practice in Elmhurst, Illinois, he is a Diplomate of the American Board of Orthodontics and an internationally recognized educator, presenting to thousands of orthodontists on subjects such as efficient treatment, esthetics, leadership, and creating a culture of excellence.
Michael Bicknell, DDS, MS, earned his DDS and completed a residency in orthodontics at the University of Illinois at Chicago College of Dentistry where he also received a MS in oral biology. He is a former clinical instructor at the university and continues his involvement there by lecturing to dental students and orthodontic residents throughout the year. In private practice in Elmhurst, Illinois, he is a Diplomate of the American Board of Orthodontics and an internationally recognized educator, presenting to thousands of orthodontists on subjects such as efficient treatment, esthetics, leadership, and creating a culture of excellence.
Disclosure: Dr. Bicknell is a Damon™ System Mentor.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
