Drs. William J. Sweeney Jr., Daniel Rinchuse, Donald Rinchuse, Thomas Zullo, and Bryan King share insights into orthodontic patients’ perceptions
Objective
The aim of this study was to gain insight into the perceptions of orthodontic patients with regard to comfort, ease of speaking, salivary flow, and satisfaction while undergoing the initial stages of orthodontic treatment using Invisalign® aligners.
Methods
Patients initiating orthodontic treatment using Invisalign aligners at a private ortho-dontic practice were surveyed using a visual analog scale (VAS) over the initial course of treatment. The first survey was completed when patients were given their initial aligners. They were surveyed again at each of their next two routine appointments.
Results
Forty of the 72 patients who initially participated in the study completed surveys at all three time points. These patients indicated that they felt the aligners were moderately comfortable, and this changed little over the course of treatment. Patients reported they felt they could generally speak well while wearing the aligners, and this also changed little during treatment. On average, patients initially reported their mouths felt neither extremely dry nor extremely wet with only a minor increase in dryness over time. Finally, patient’s satisfaction began high and increased during the first time period and then remained constant through the final time point.
Conclusion
Despite what patient’s may believe after searching the Internet or talking with friends, treatment using Invisalign aligners is a relatively positive one. Patients report the aligners are comfortable, do not interfere with speaking, and do not cause excessive dryness or salivation. Patients also report being satisfied with the experience during their initial phase of treatment.
Introduction
“Perception is reality.” — Lee Atwater
A positive experience using orthodontic aligners may lead to better acceptance and compliance, which may lead to enhanced results. Accurately anticipating patients’ experiences may improve practitioners’ ability to communicate with patients regarding what might be expected during treatment. Further, it may also be helpful to be able to advise patients if they can expect these feelings to change throughout treatment. Because various companies use different materials for aligner fabrication, this study used only Invisalign aligners from Align Technologies, Inc.
A Google® search in April of 2013 using the phrase “Invisalign problems” revealed online testimonies of Invisalign aligners being associated with the sensation of a dry mouth, excessive salivation, impaired speech, and general discomfort. Further refining the Google query as “Invisalign Dry Mouth,” “Invisalign Excess Saliva,” “Invisalign Speech,” “Invisalign Pain,” and “Invisalign Discomfort” quickly revealed that there are numerous instances of patients proclaiming perceived adverse experiences while using Invisalign aligners. Although not an exhaustive review, a PubMed search was conducted to investigate publications regarding the use of Invisalign being associated with sensations of: dry mouth, excess salivation, impaired speech, or discomfort. Boolean searches of PubMed were conducted using “Invisalign AND” in conjunction with the following terms; the number of associated results is in parenthesis: Xerostomia (1), Dry mouth (1), Salivation (0), Speech (2), Comfort (0), Discomfort (1), Satisfaction (6), Perception (1), and Experience (4).
Background
Xerostomia
The diagnosis of xerostomia can be through questioning the patient, salivary output studies, or imaging. Irrespective of whether scientific testing provides objective results, a patient’s report of xerostomia may indicate the need for palliative therapy to provide symptomatic relief.1 Thus, xerostomia, as the subjective condition relevant to this study, can only be ascertained through direct questioning of patients.2
In addition to objective clinical success, orthodontists would also like their patients to have a positive experience. Decreased salivary function could have an impact on the person’s quality of life.3 For the purposes of this study, the definition of xerostomia was taken from the American Dental Association as follows: “Xerostomia is defined as the subjective complaint of dry mouth that may result from a decrease in the production of saliva.”1 Though it could be argued that testing is required to determine if xerostomia is actually present, throughout the literature, xerostomia is considered the “subjective sensation of dry mouth.”4 It has been estimated that a 50% reduction in salivary secretion needs to occur before xerostomia becomes apparent,5 and xerostomia is estimated to affect one in every 10 dental patients.3 Symptoms may be due to a reduction in the quality of saliva produced, the actual composition of saliva, or both. Xerostomia, as defined by the American Dental Association is a subjectively perceived condition with no objective evidence of a change in salivary quantity or quality, is relevant for this study.1
Historically, head-and-neck radiation therapy was considered the most common cause of xerostomia and salivary gland hypofunction. Systemic diseases such as Sjogren’s syndrome, HIV, and others are also associated with xerostomia. Currently, medications have emerged as the most common cause.3 According to Villa, et al., medication usage and age are highly significant risk factors for dental patients reporting xerostomia,6 and medications may be associated with a feeling of dry mouth despite normal saliva production.7 It is important to note that the association with age may simply be due to the increased likelihood that patients may be taking medications as they age. Specific PubMed searches using “Invisalign AND” with the following terms returned the subsequent results: Xerostomia (1), Dry mouth (1), and Salivation (0).
Hypersalivation
Patients may also present with hypersalivation, also known as ptyalism or sialorrhea. Increased salivary flow may be due to a medical condition such as a neurologic disorder.8 The use of certain medications such as the antimuscarinic agent glycopyrrolate may also stimulate salivary flow.9 Medication such as Salvart Synthetic Saliva may also be used as a salivary substitute.10 Additionally, a relative feeling of excess salivary flow may be due to the patient’s inability to clear a normal amount of saliva, as is the case for patients with amyotrophic lateral sclerosis.11
Searches of PubMed to find articles pertaining to hypersalivation’s possible connection to Invisalign revealed publications relevant to the topic as follows: Hyper-salivation (1480) alone as well as “Medication AND” the following: Hypersalivation (132), Increased Salivation (2165), Ptyalism (1220), Sialorrhea (1173), Sialorrhea drug therapy (277), Saliva substitutes (2568), Artificial saliva (2456). Further, PubMed was searched using “Invisalign AND” and the following was found: Saliva (4), Salivary (0), Salivation (0), Ptyalism (0), Sialorrhea (0), and Hyper-
salivation (0).
Discomfort
Discomfort associated with the use of Invisalign aligners may be due to the pressures applied to the teeth or physical irritation of soft intraoral tissues. Owen addressed soft tissue irritation in a case report of his own personal treatment experience.12 Tucany, et al., reported that teenage patients “seldom or never experienced discomfort.”13 A study of 54 consecutive patients by Nedwed and Miethke found that patients “do not suffer much impairment” while using Invisalign aligners.14 Miller, et al., reported that “adults treated with Invisalign aligners experienced less pain and fewer negative impacts on their lives during the first week of orthodontic treatment than did those treated with fixed appliances.”15
Shalish, et al., compared the level of discomfort experienced by patients using labial brackets,lingual brackets, and Invisalign aligners. The results indicated that Invisalign aligners were better tolerated than both labial and lingual brackets.16 In the studies of both Miller, et al., and Fujiyama, et al., it was reported that the discomfort experienced by patients using Invisalign aligners to be less than those using traditional labial appliances.15,17 PubMed searches were performed for “Invisalign AND” with the following results: Pain (7), Comfort (0), and Discomfort (2).
Speech
Prospective Invisalign patients may fear potential difficulty speaking while wearing aligners. Owens mentions that he himself suffered compromised speech for a short time after beginning Invisalign therapy when reporting his own experience as a patient.12 Nedwed and Miethke’s investigation found that patients “become accustomed to the aligners very quickly and do not suffer much impairment.”14 Results of a PubMed search for ”Invisalign AND” combined with the following are Speech (2), Speaking (1), and Talking (2).
Satisfaction
Nedwed and Miethke reported that “98% of patients were satisfied with the progress of therapy”14 in their study. Schaefer and Braumann reported that 84% of their subjects were “very satisfied” with the results of treatment and 16% were “satisfied.”18 The PubMed search criteria and number of results for “Invisalign AND” the following are Satisfaction (6), Satisfied (1), and Happy (0).
Aim
The aim of this study was to investigate the perceptions of patients with regard to comfort, ease of speaking, salivary flow, and satisfaction while undergoing the initial stages of orthodontic treatment using
Invisalign aligners.
Method
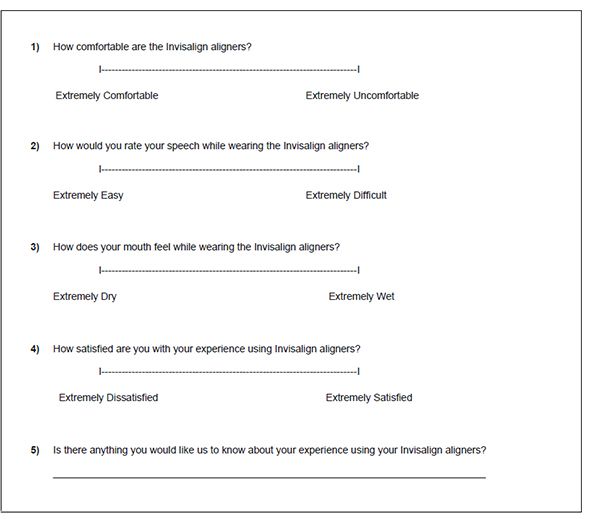
Seventy-two consecutively treated patients beginning treatment in a private orthodontic practice, who met the inclusion criteria, began this pilot study by completing the initial survey (Figure 1) at time T1, their first appointment with the initial aligners. Of these 72 patients, 40 patients completed surveys at all three time points during the study. Patients were surveyed at the beginning of treatment after wearing their initial aligners for a few minutes (T1); again at their second routine follow-up appointment (T2); between 14-91 days, with a mean of 34.2 days; and finally, at their third routine follow-up appointment (T3) between 64-169 days, with a mean of 106.9 days.
A relatively large number of patients who completed the survey at T1 did not complete surveys at either T2 or T3 or both. This was due to the clinical staff charged with collecting the surveys inadvertently forgetting to have the patients complete the survey at either T2 or T3. The time constraints of the private practice’s schedule also precluded the completion of some surveys. If all three time points were not complete for a particular patient, no surveys for that patient were included in the study. This resulted in the loss of 44% of the subjects who initially agreed to participate in the study.
Each patient was asked to indicate his/her level of perceived intraoral comfort, dryness/wetness, ability to speak, and satisfaction with his/her experience with the Invisalign aligners using a visual analog scale (VAS) during routine appointments at time points T1, T2, and T3. Patients were also given the opportunity to inform the doctor or staff of any other issues they felt were important. Those personnel administering the surveys were instructed to avoid giving any advice, opinions, or in any way influencing the patient’s perceived experience.
Align Technologies has changed the material used in aligner fabrication over time, which may lead to different patient experiences currently when compared to years ago. “SmartTrack” is the third generation of material used to fabricate Invisalign aligners and was utilized for all patients in this study.
Patients were excluded from the study if they were under 18 years of age or had had any predisposing conditions such as a history of radiation, chemotherapy, systemic disease, medication, or medical conditions that may increase the likelihood of xerostomia, ptyalism, speech impediments, or discomfort.
The Multivariate and Univariate Tests, Pairwise Comparison and Mean Value Estimate were performed using IBM SPSS v.23 software.
Results
The overall Multivariate Test was performed to determine if there were overall differences (changes over time) for comfort, speech, salivary flow, and satisfaction with the experience of using aligners. The overall significance level (p-value) was 0.013 with an f-value of 3.019 leading clinicians to conclude that there were differences (changes over time). This is of statistical importance, but not of much practical importance since it does not provide information regarding which of the four measures changed over time.
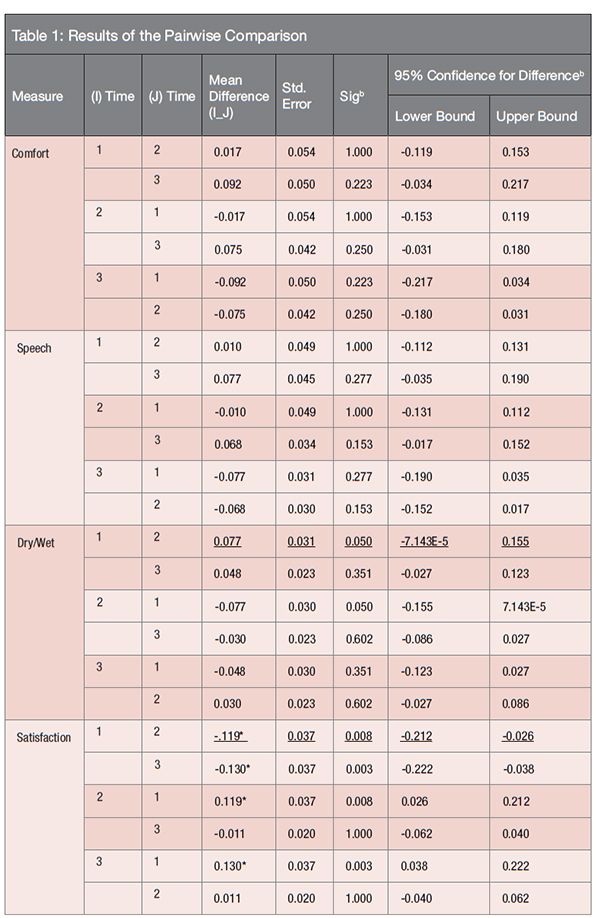
* The mean difference is significant at the .05 level. Adjustment for multiple comparisons: Bonferroni
The Univariate Test was performed to determine which individual measures changed over time. The significance level (p-value) for comfort and speech, which were 0.145 and 0.150, respectively, are greater than 0.05 leading clinicians to conclude that there were no significant changes over time for these measures. Dry/wet and satisfaction do have significance levels (p-values) of 0.025 and 0.000, respectively, which are less than 0.05, indicating there are differences over time.
Determining exactly where the changes over time occurred required the use of both a Pairwise Comparison (Table 1) and Mean Value Estimates (Table 2). Again, as would be expected from the Univariate Tests results, no significant differences (changes over time) were found for comfort and speech using the Pairwise Comparisons between any time points (T1-T2), (T1-T3), or (T2-T3).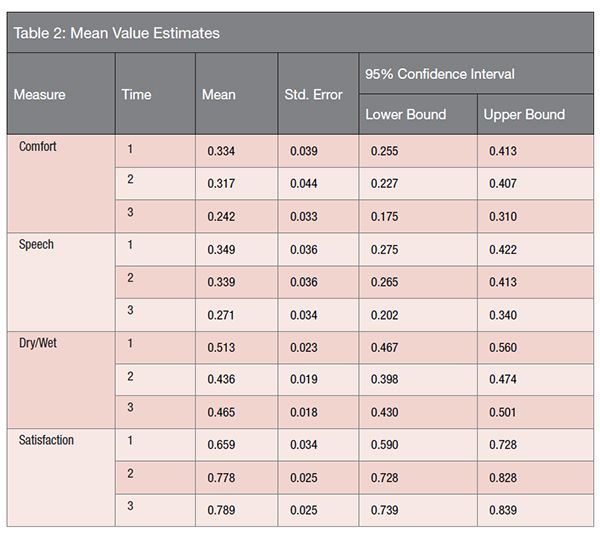
Looking at the comparisons for satisfaction, it can be seen that differences between T1-T2 and T1-T3 were statistically significant (p = 0.008 and p = 0.003, respectively) while the difference between T2-T3 is not significant. Since the mean differences are negative (meaning the second value is larger), it can be concluded that satisfaction increases significantly between T1-T2 and between T1-T3, but there is no significant increase between T2-T3.
The findings for dry/wet are a little more statistically complex. The Univariate Tests for dry/wet show statistically significant differences across the time points. Also, the table for pairwise comparisons shows a significance value of 0.050 for the difference between T1-T2 for dry/wet. However, the Mean Difference value does not have an asterisk to indicate “The mean difference is significant at the 0.05 level.” It should be noted that, although the value printed out is 0.05, the actual value is 0.0503, which is very close. When controlling for Type II error, in this case pairwise error rate, one must conclude that none of the pairwise comparisons (1 versus 2, 1 versus 3, or 2 versus 3) are significantly different from each other.
Discussion
Patients with extreme or atypical experiences using Invisalign aligners may not be the norm and may be more likely to vocalize or post to the Internet their experiences and, thus, may be overrepresented. With more evidence, especially high-quality evidence, practitioners would be in a position to confidently inform Invisalign patients of realistic expectations and not anecdotal information found on the Internet.
From the result of this study, patients can expect to be reasonably comfortable with little speech impairment. While statistically insignificant, patient’s initial slight dis-comfort and speech inhibition did technically improve slightly during the initial phases of treatment. Some patients have also indicated they feel the edges of the aligners were sharp when asked if they would like to report anything specific. Simply buffing the edges of the aligners or an improved manufacturing process may alleviate this issue.
The results of the study show a dry- or wet-mouth feel is almost exactly in the middle of the visual analog scale. This may indicate that there is no difference from what patients perceive as normal. Further studies to isolate patients into subgroups of those experiencing xerostomia from those experiencing ptyalism may better indicate the experience and associated changes over time. Finally, patients undergoing orthodontic treatment using Invisalign aligners may expect that they will be satisfied with their experience. They will also feel an initial increase in the level of satisfaction that will continue through the initial phase of treatment.
Schaefer and Braumann reported that, while patients could not be objectively shown to have dry mouths, their subjects did report the occasional feeling of dry mouth, particularly over the first 3 to 4 months.18 However, this subjective feeling of dry mouth was reported to have hardly influenced the patients’ quality of life and was thought to be attributable to the patients’ heightened awareness of their oral condition. Similarly, Schaefer and Braumann’s subjects initially reported difficulties with certain pronunciations and sensations of pain but with little impact on their lives. Finally, Schaefer and Braumann’s subjects reported being satisfied with their results. Likewise, Nedwed and Miethke reported that, while there may be some mild transient pain or speech impairment, their subjects reported these issues quickly dissipated and were of little relevance leading to a high level of patient satisfaction with aligner therapy.14
Limitations
This pilot study had a relatively small sample size, and the length of the study could be extended. Patients were followed for the first three appointments, and patient experiences may change after long-term wear over the full course of treatment. Thirty-two of the initial 72 subjects who initially participated did not complete all three surveys, leaving only 40 subjects who completed all three surveys. This study also did not investigate the effects of wearing Invisalign aligners on patients under the age of 18 years of age. Patients under the age of 18 years old may have different responses to the aligners than adults. Subjects were not segregated into groups according to occlusal classification.
This pilot study focused on publications found through searching PubMed as a preliminary investigation. A more exhaustive review of the literature would include MEDLINE®, Embase®, and the Cochrane Library, in addition to AAO resources and hand searching. These additional search methods may reveal additional research. A confounder may be that some patients with undiagnosed medical conditions or those taking medications may have inadvertently been included in this study. All patients in the study came from the same private practice and may have been influenced in ways that were not determined. Because the patients were aware their answers were being tracked, they may have experienced a Hawthorne effect, also referred to as the observer effect.
Clinical implications
This pilot study and the literature cited in this paper may allow clinicians to be optimistic about the minor negative patient experiences with Invisalign therapy.
Conclusion
This study followed patients using Align Technologies’ Invisalign brand aligners during their initial phase of treatment. The findings indicate there is little clinically significant effect on comfort, speaking, the level of dryness, or excess salivation perceived by the patient. Perhaps most importantly, the majority of patients were satisfied; only one patient reported being dissatisfied with the experience of using the Invisalign aligners.
- Guggenheimer J, Moore PA. Xerostomia: Etiology, recognition and treatment. J Am Dent Assoc. 2003;134(1):61-69.
- Hopcraft, MS, Tan C. Xerostomia: an update for clinicians. Aust Dent J. 2010;55(3):238-244.
- ADA Council on Scientific Affairs. Artificial salivas. Xerostomia. J Am Dent Assoc. 2001:132(2):1720-1721.
- Furness S, Bryan G, McMillan R, Birchenough S, Worthington HV. Interventions for the management of dry mouth: non-pharmacological interventions. Cochrane Database Syst Rev. 2013;9.
- Dawes C. Physiological factors affecting salivary flow rate, oral sugar clearance, and the sensation of dry mouth in man. J Dent Res. 1987;66:648-53.
- Villa A, Polimeni A, Strohmenger L, Cicciù D, Gherlone E, Abati S. Dental patients’ self-reports of xerostomia and associated risk factors. J Am Dent Assoc. 2011;142(7):811-816.
- Furness S, Worthington HV, Bryan G, Birchenough S, McMillan R. Intervention for the management of dry mouth: topical therapies. Cochrane Database Syst Rev. 2011;12.
- Boyce HW, Bakheet MR. Sialorrhea: a review of a vexing, often unrecognized sign of oropharyngeal and esophageal disease. J Clin Gastroenterol. 2005;39(2):89-97.
- Blissit KT, Tillery E, Latham C, Pacheco-Perez J. Glycopyrrolate for treatment of clozapine-induced sialorrhea in adults. Am J Health Syst Pharm. 2014;71(15):1282-1287.
- Dental Product Spotlight. Artificial Salivas. J Am Dent Assoc. 2001;132(12):1720-1.
- Young CA, Ellis C, Johnson J, Sathasivam S, Pih N. Treatment for sialorrhea (excessive saliva) in people with neuron disease/amyotrophic lateral sclerosis. Cochrane Database Syst Rev. 2011; 5(pub2).
- Owen AH 3rd. Accelerated Invisalign treatment. J Clin Orthod. 2001;35(6):381-385.
- Tuncay O, Bowman SJ, Amy B, Nicozisis JT. Aligner Treatment in the teenage patient. J Clin Orthod. 2013;47(2):115-119.
- Nedwed V, Miethke RR. Motivation, acceptance and problems of Invisalign patients. J Orofac Orthop. 2005;66(2):162-173.
- Miller KB, McGorray SP, Womack R, Quintero JC, Perelmuter M, Gibson J, Dolan TA, Wheeler TT. A comparison of treatment impacts between Invisalign aligner and fixed appliance therapy during the first week of treatment. Am J Othod Dentofacial Orthop. 2007:131(3):302e1-9.
- Shalish M, Cooper-Kazaz R, Ivgi I, Canetti L, Tsur B, Bachar E, Chaushu S. Adult patients’ adjustability to orthodontic appliances. Part I: a comparison between Labial, Lingual, and Invisalign. Eur J Orthod. 2012;34(6):724–730.
- Fujiyama K, Honjo T, Suzuki M, Matsuoka S, Deguchi T. Analysis of pain level in cases treated with Invisalign aligner: comparison with fixed edgewise appliance therapy. Prog Orthod. 2014;22:15:64.
- Schaefer I, Braumann B. Halitosis, oral health and quality of life during treatment with Invisalign® and the effect of low-dose chlorhexidine solution. J Orofac Orthop. 2010;71(6):430-441.
Stay Relevant With Orthodontic Practice US
Join our email list for CE courses and webinars, articles and mores
